What's Here? - Table of Contents
Short answer: yes—for many roles and career goals. The CCC-SLP (ASHA’s Certificate of Clinical Competence) signals nationally standardized training and competence across three pillars: CAA-accredited graduate education, a passing Praxis® SLP score, and a supervised Clinical Fellowship. Employers and payers recognize it. Many hospitals, rehab networks, and large school systems require or strongly prefer it. While a state license is the legal permission to practice, the CCC-SLP is a portable professional credential that expands options, unlocks supervision privileges, and strengthens long-term credibility.
What this means in practice:
Required in many medical settings; often preferred in schools and private practice because it streamlines credentialing and boosts trust with families, teams, and payers.
Career advantage: eligibility to supervise CFs and students, easier mobility between states and settings, and a stronger signal on resumes, LinkedIn, and credentialing packets.
Trade-offs: initial and renewal fees, ongoing CEU requirements, and documentation discipline. For SLPs with stable, district-specific roles, state license alone may be sufficient—but it narrows portability and can limit supervision/leadership paths.
When to prioritize CCC-SLP now:
Targeting hospitals, SNFs, outpatient clinics, or multi-state opportunities
Planning to supervise CFs or students, lead teams, or move into admin
Building a private practice/telepractice that joins payer panels
When you might delay:
Locked into a district role that does not require CCC and offers no pay/role differential
Short-term constraints on fees or CE that make immediate certification impractical
Bottom line: If the roadmap includes medical settings, payer credentialing, supervision, leadership, or geographic flexibility, prioritize CCC-SLP. If the plan is a long runway in one district with stable rules and no desire to supervise, a state license may cover the essentials—for now.
CCC-SLP stands for Certificate of Clinical Competence in Speech-Language Pathology, a nationally recognized professional certification awarded by ASHA. It’s a simple idea with real weight: standardized proof of readiness to practice at a high level—recognized by employers, payers, and peers across settings and states.
What the CCC-SLP signals
Accredited education: Completion of a CAA-accredited master’s program in speech-language pathology.
Knowledge benchmark: A passing score on the Praxis® SLP examination.
Real-world competence: Successful completion of a mentored Clinical Fellowship (CF) that demonstrates independent clinical readiness.
Professional standards: Agreement to ASHA’s Code of Ethics and ongoing adherence to practice expectations.
What it does (in practical terms)
Sets a national bar so HR teams, hospitals, school systems, and payers can trust the training behind the credential.
Expands options by making qualifications legible across settings (medical, school, private practice, telepractice).
Enables supervision in many contexts (e.g., CF supervision), supporting leadership growth and team development.
What it’s not
Not a state license. Licensure is the legal permission to practice, issued by a state board. CCC-SLP is a professional credential that complements—not replaces—state licensure. (We’ll unpack differences next.)
Why programs and employers care
It reduces risk (consistent minimum standards).
It simplifies credentialing (clear evidence of education, exam, and supervised practice).
It supports quality (ethics framework + continuing education maintenance requirements).
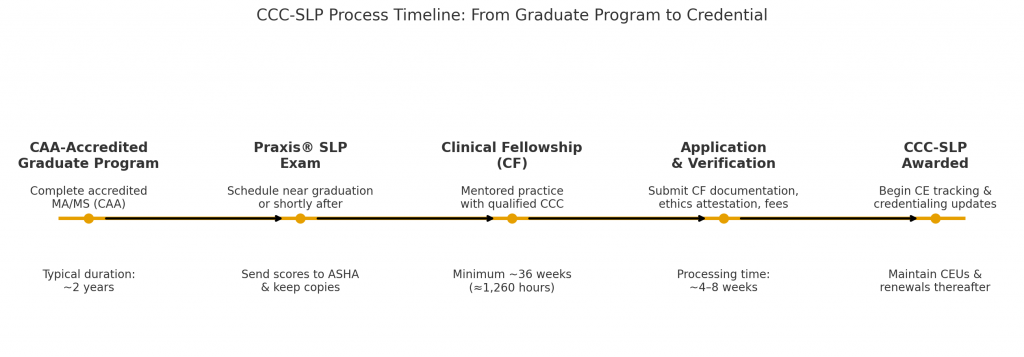
The path is straightforward: complete an accredited degree, pass Praxis®, finish a mentored Clinical Fellowship, then submit a clean, complete application. Do each piece on time, keep documentation tight, and the credential follows.
What counts: MA/MS in SLP from a CAA-accredited program with required academic and clinical hours.
When to do it: 4–6 terms for most students; confirm your program’s CAA status before day one.
Save this: Final transcript (degree posted), clinic hour verification, any remediation plans.
Pitfalls: Assuming “institutional accreditation” equals CAA; missing prerequisite leveling requirements that delay graduation.
What counts: A passing Praxis® SLP score sent to ASHA and your state (as needed).
When to do it: Late in the final term or immediately after graduation to keep momentum into the CF.
Save this: Unofficial score on test day; official score report confirmation once posted.
Pitfalls: Testing too early without content mastery; forgetting to designate ASHA as a recipient; name mismatches across accounts.
What counts: Minimum ~36 weeks (~1,260 hours) of supervised practice under a qualified CCC-SLP mentor, with periodic formal evaluations.
When to do it: Start as soon as you secure an eligible CF position; plan evaluations from day one.
Save this: CF contract/offer letter noting mentor’s CCC status, evaluation forms, hour logs, setting details.
Pitfalls: Mentor without current CCC; fragmented sites without proper oversight; incomplete or inconsistent hour logs that slow verification.
What counts: ASHA application, verification of education, Praxis® score, CF documentation, ethics attestation, and fees.
When to do it: Immediately after the CF is verified; earlier prep shortens turnaround.
Save this: Copies of every submission, payment receipt, and confirmation emails.
Pitfalls: Missing signatures, wrong forms for multi-site CFs, name discrepancies, or expired mentor credentials.
What counts: Ongoing CEUs per ASHA requirements, including any ethics component; timely renewal.
Save this: Centralized CE log, certificates, and renewal confirmations—separate from state CE files.
Pitfalls: Assuming state CE = ASHA CE; losing certificates; letting renewal dates drift.
Think of these as three separate lanes that often run in parallel:
CCC-SLP = national professional credential (ASHA) that signals standardized competence.
State SLP License = state board’s legal permission to practice.
School Credential = state department of education or district authorization to work in K–12.
Both employers and payers read these lanes differently. Get clear now and hiring, credentialing, and reimbursement move faster later.
| Dimension | CCC-SLP (ASHA) | State SLP License | School Credential (K–12) |
|---|---|---|---|
| Primary purpose | National professional certification signaling education, exam, CF, and ethics | Legal authorization to practice SLP in that state | Authorization to work as an SLP in public schools (state/district rules) |
| Governing body | ASHA | State licensing board | State department of education / district HR |
| Scope | Professional standard recognized nationally | State-specific practice authority (all settings in that state) | K–12 setting within that state/district |
| Portability | Portable signal across states and employers | Not portable; requires new license when moving states | Not portable; varies by state/district rules |
| Typical employer view | Often required/strongly preferred in medical and large systems | Always required to practice in that state (outside K–12 exceptions) | Often sufficient for school roles; CCC may still be preferred |
| Payer & network credentialing | Frequently simplifies credentialing and enhances trust | Required if billing in that state | Usually not applicable unless billing outside school systems |
| Supervision eligibility | Commonly required to supervise CFs and many students | Varies by state rule | Varies by district/state |
| Maintenance | ASHA renewal + CE/ethics | State renewal + CE (separate from ASHA) | State/district renewal; PD requirements vary |
| If it lapses | Lose professional credential; may impact roles/supervision | Lose legal ability to practice in that state | Lose school eligibility per state/district rules |
Licensure is non-negotiable for clinical practice in a state; treat it as the floor. See state SLP licensing requirements.
CCC-SLP is leverage—opens doors in hospitals, payer-credentialed clinics, and leadership/supervision tracks.
School credentials can get a clinician into classrooms quickly; CCC still strengthens mobility and pay negotiations.
Medical/SNF/outpatient or multi-state moves? Prioritize CCC-SLP + state license.
Stable K–12 role in one district? School credential + state license may cover immediate needs, but CCC preserves optionality.
Plan to supervise CFs or students? CCC-SLP typically required.
License only: legal but less portable; potential ceiling on supervision/advanced roles.
School credential only: limits movement to medical/private settings; may reduce negotiation leverage.
CCC only (no license): not sufficient to practice—still need the state license where services are delivered.
Credentials drive access. Employers, payers, and districts read them differently—so the play is to match the credential stack to the setting. Use this matrix to decide what’s essential now versus what can wait.
| Setting | Typical expectation | Why it matters | Recommended credential stack to apply with |
|---|---|---|---|
| Hospitals / Acute Care | CCC-SLP often required; always need state license | Medical staff bylaws & payer credentialing favor standardized competence | State license + CCC-SLP (+ facility onboarding, immunizations, BLS) |
| Rehab / SNF | Frequently required or strongly preferred | Third-party payers and corporate QA programs lean on CCC for consistency | State license + CCC-SLP (+ dysphagia competencies as applicable) |
| Outpatient / Private Clinics | Often required or preferred, especially if paneling with insurers | Network credentialing and referral partners value portable standards | State license + CCC-SLP (+ payer panel docs, liability coverage) |
| Telepractice | Commonly preferred; depends on platform and payer mix | Multi-state work and insurance billing favor CCC-SLP portability | Licenses for each service state + CCC-SLP (+ HIPAA/tech compliance) |
| Early Intervention (Part C) | Varies by state; CCC often preferred | State vendor enrollment, Medicaid policies, supervision rules | State license (+/- CCC-SLP depending on state vendor standards) |
| K–12 Schools | Usually school credential + state license; CCC is preferred in many districts | Ed-department rules govern schools; CCC adds mobility, pay leverage, supervision eligibility | State license + school SLP credential (+/- CCC-SLP for advancement) |
| Home Health | Often preferred (some agencies require) | Payer audits and safety policies emphasize standardized training | State license + CCC-SLP (+ home-health orientation) |
| University / Research / Admin | Mixed; CCC frequently expected for clinical supervision | Accreditation and CF/student supervision privileges | State license (if providing care) + CCC-SLP for supervision roles |
If insurers are involved, expect CCC-SLP to be required or strongly preferred.
If supervising CFs or students is on the roadmap, plan on CCC-SLP.
If staying in one district with a stable school credential and no supervision duties, licensure + school credential may cover the role—but portability and advancement narrow.
Always verify at three levels: state board requirements, employer policy, and payer/medical staff credentialing rules.
Medical, SNF, outpatient, telepractice, home health? Prioritize CCC-SLP now.
School-only, long horizon, no supervision? CCC-SLP can be deferred—with eyes open to limits on mobility and panels.
Thinking leadership or precepting? Secure CCC-SLP to unlock supervision credentials.
Make the call in 60 seconds—answer these five questions:
Primary setting for the next 1–3 years?
Hospitals/SNF/outpatient/telepractice → Prioritize CCC-SLP now.
Single district K–12 with stable rules → May defer, eyes open to limits.
Payer mix involved (insurance/Medicaid/Medicare)?
Yes → CCC-SLP typically required or strongly preferred.
Will supervision/leadership matter?
Plan to supervise CFs or students, lead a team, or move into admin → Get CCC-SLP.
Geographic mobility needed?
Multi-state options or telepractice across states → Get CCC-SLP for portability.
Employer/district policy today?
If a posting, HR policy, or medical staff bylaws list CCC-SLP → Non-negotiable.
Credential stack by scenario:
Medical/SNF/outpatient/tele: State license + CCC-SLP (+ immunizations/BLS, payer docs).
K–12, stable district, no supervision: State license + school credential (CCC-SLP optional now).
Private practice building payer panels: State license + CCC-SLP (+ liability coverage, NPI, panels).
